 New
New How to Take Blood Pressure
CPDTime.
19m
Published: 18 June 2023


Published: 18 June 2023
There are many ways to measure blood pressure. The most simple and common way to measure blood pressure is the brachial artery occlusion method, commonly known as the cuff.
The accuracy of the measurement depends on correct cuff sizing and operator use. It can be done automatically, but once again, training is required for automatic use.
Blood pressure (BP) is a measure of the pressure exerted by the blood as it flows through the arteries. It is measured in millimetres of mercury (mmHg.
The purpose of taking a blood pressure measurement may be to:
Blood pressure measurements take into account:
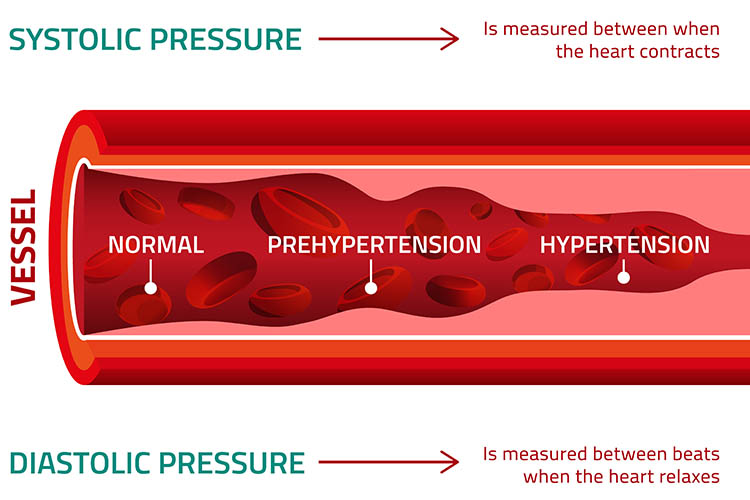
A normal systolic pressure for an adult is less than 120 mmHg, and a normal diastolic is less than 80 mmHg (NIA 2022).
Influencing factors include but are not limited to:
Blood can only be heard through a stethoscope if it is turbulent. As the cuff is inflated, the artery is compressed, making the blood flow through the artery turbulent. When the artery is completely closed, there is no blood flow and no sound. As pressure in the cuff is reduced, the point at which the artery is open just enough to let the blood pass is the systolic blood pressure.
This is detected by turbulent blood flow heard through the stethoscope. The resulting turbulence produces characteristic tapping sounds known as Korotkoff sounds. As pressure in the cuff is further reduced, the vessel will once again be completely open and non-turbulent. At this point, no more Korotkoff sounds are heard and diastolic blood pressure has been reached.
Korotkoff sounds are generated when a blood pressure cuff changes the flow of blood through the artery. These sounds are heard through either a stethoscope or a doppler that is placed distal to the blood pressure cuff.
There are five distinct phases of Korotkoff sounds:
| Phase 1: A sharp tapping. | This is the first sound heard as the cuff pressure is released. This sound provides the systolic pressure reading. |
| Phase 2: A swishing/whooshing sound. | Swishing sounds as the blood flows through blood vessels as the cuff is deflated. |
| Phase 3: A thump (softer than phase 1). | Intense thumping sounds that are softer than phase 1 as the blood flows through the artery but the cuff pressure is still inflated to occlude flow during diastole. |
| Phase 4: A softer, blowing, muffled sound that fades. | Softer and muffled sounds as the cuff pressure is released. The change from the thump of phase 3 to the muffled sound of phase 4 is known as the first diastolic reading. |
| Phase 5: Silence. | Silence that occurs when the cuff pressure is released enough to allow normal blood flow. This is known as the second diastolic reading. |
Initial preparation:
Choose a measurement site:
Position the patient either sitting, standing, supine or prone depending on your choice of measurement site.
Palpate the artery to determine the systolic BP:
Position the stethoscope over the brachial artery and use the bell side.
Auscultate the BP:
If a repeat is necessary, wait two minutes before inflating the cuff again.
If required for your assessment, repeat the procedure on the other arm or in a standing position for a postural BP.
Remove the cuff.
Advise the patient of the result.
Clean and return the equipment.
Document.
BP is recorded as a fraction, with the top number representing the systole and the bottom number representing the diastole. If first and second diastolic are recorded, the first diastolic is written over the second, i.e. 120/90/80.
Documentation post the assessment is essential and should include the location the BP was taken and any factors that may have impacted the result. Furthermore, it is important that healthcare professionals note that drastic changes in BP can be a sign of clinical deterioration.
Question 1 of 3
Swishing occurs in which phase of Korotkoff sounds?


Ausmed Education is a Trusted Information Partner of Healthdirect Australia. Verify here.