
In 2026, the workforce shortage in Australian aged care has changed shape. It is no longer a recruitment problem that can be solved by hiring harder, paying more, or running a better careers campaign. It is a structural mismatch between the work the sector needs to do and the workforce available to do it.
That mismatch has been widening for years. The Royal Commission into Aged Care Quality and Safety (2021) established the moral case for investment in workforce capability. The Aged Care Act 2024 and the Strengthened Aged Care Quality Standards have translated that case into binding obligations (Aged Care Quality and Safety Commission, 2025; Department of Health, Disability and Ageing, 2025a). The 24/7 registered nurse requirement, the care minutes mandate, and the forthcoming Aged Care Worker Registration Scheme have set a new floor for what is expected, not what is exceptional.
For Chief People Officers, Heads of Quality and Risk, HR Managers, and L&D leaders, the question in 2026 is no longer how to fill vacancies. It is how to make every existing role more durable, how to extract more capability from every training hour, and how to position workforce investment as a board-level retention strategy rather than an operational cost.
This piece is the state of the sector, and the levers leaders can actually pull.
The 2026 picture
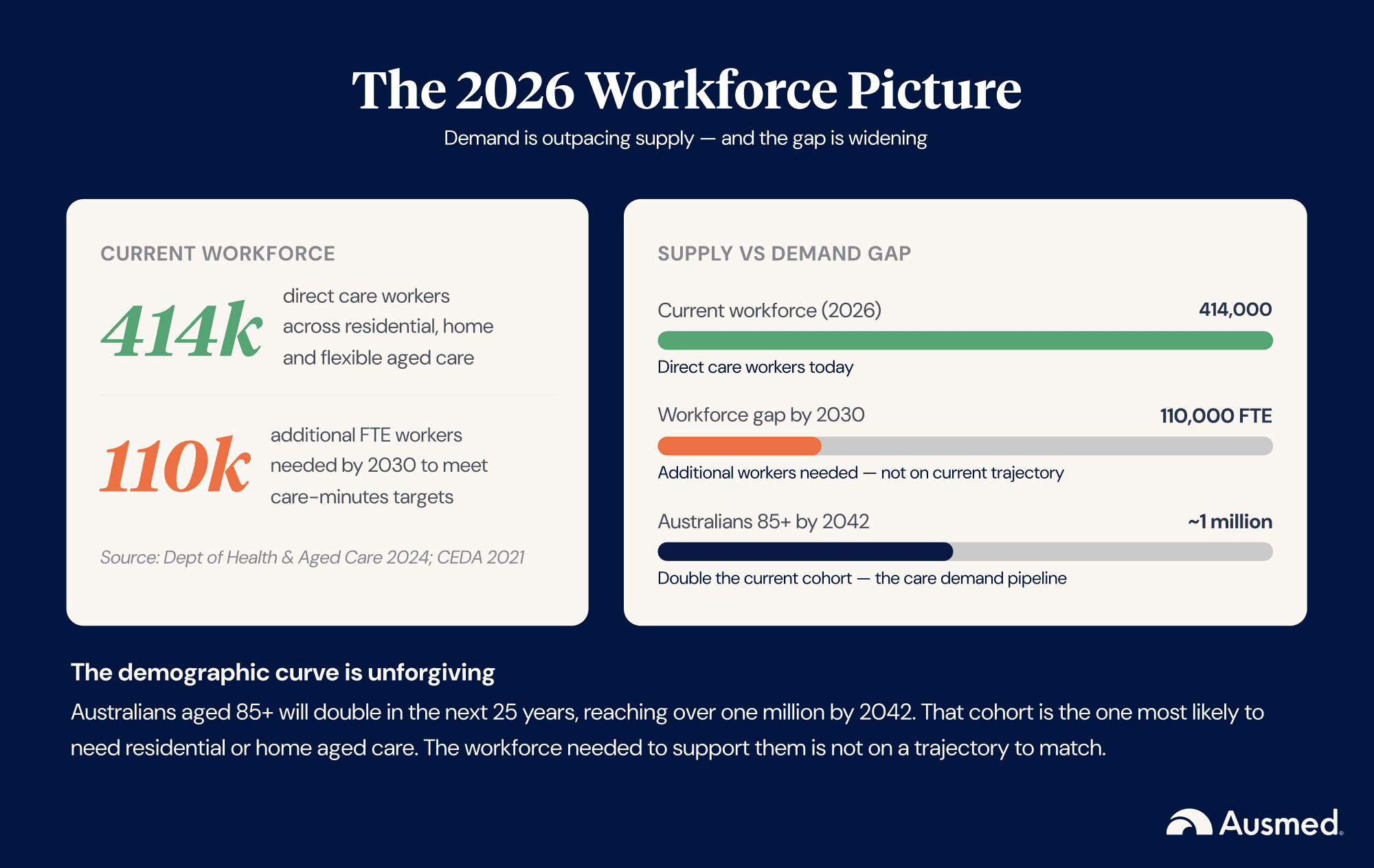
The Department of Health and Aged Care's 2023 Aged Care Provider Workforce Survey identified an estimated 414,000 direct care workers across residential, home and flexible aged care in Australia, including nurses, personal care workers and allied health professionals (Department of Health and Aged Care, 2024a). Demand is projected to outpace supply. The Committee for Economic Development of Australia and the Aged Care Workforce Industry Council have estimated that the sector needs around 110,000 additional full-time-equivalent direct care workers by 2030 to meet care-minutes targets and the demands of an ageing population (CEDA, 2021).
The Australian Bureau of Statistics projects that the number of Australians aged 85 and over will double in the next 25 years, reaching more than one million people by around 2042 (ABS, 2023). That cohort is the one most likely to need residential or home aged care. The workforce needed to support them is not on a trajectory to match.
Tenure data remains imperfect, but the Aged Care Worker Survey 2024 (which heard from over 21,000 workers) shows that 59 per cent work permanent part-time and average just 26.4 paid hours per week, and that turnover and intentions-to-leave remain the sector's most persistent operational risks (Department of Health and Aged Care, 2024b). Independent industry analysis points to high turnover, particularly in regional and remote areas where workforce attraction is hardest (Ageing Australia, 2024).
What providers know intuitively is that each of these numbers compounds the others. Lower tenure means more induction. More induction means more L&D capacity consumed. Less L&D capacity means less time for capability development. Less capability development means harder retention.
Why the shortage is compounding, not stabilising
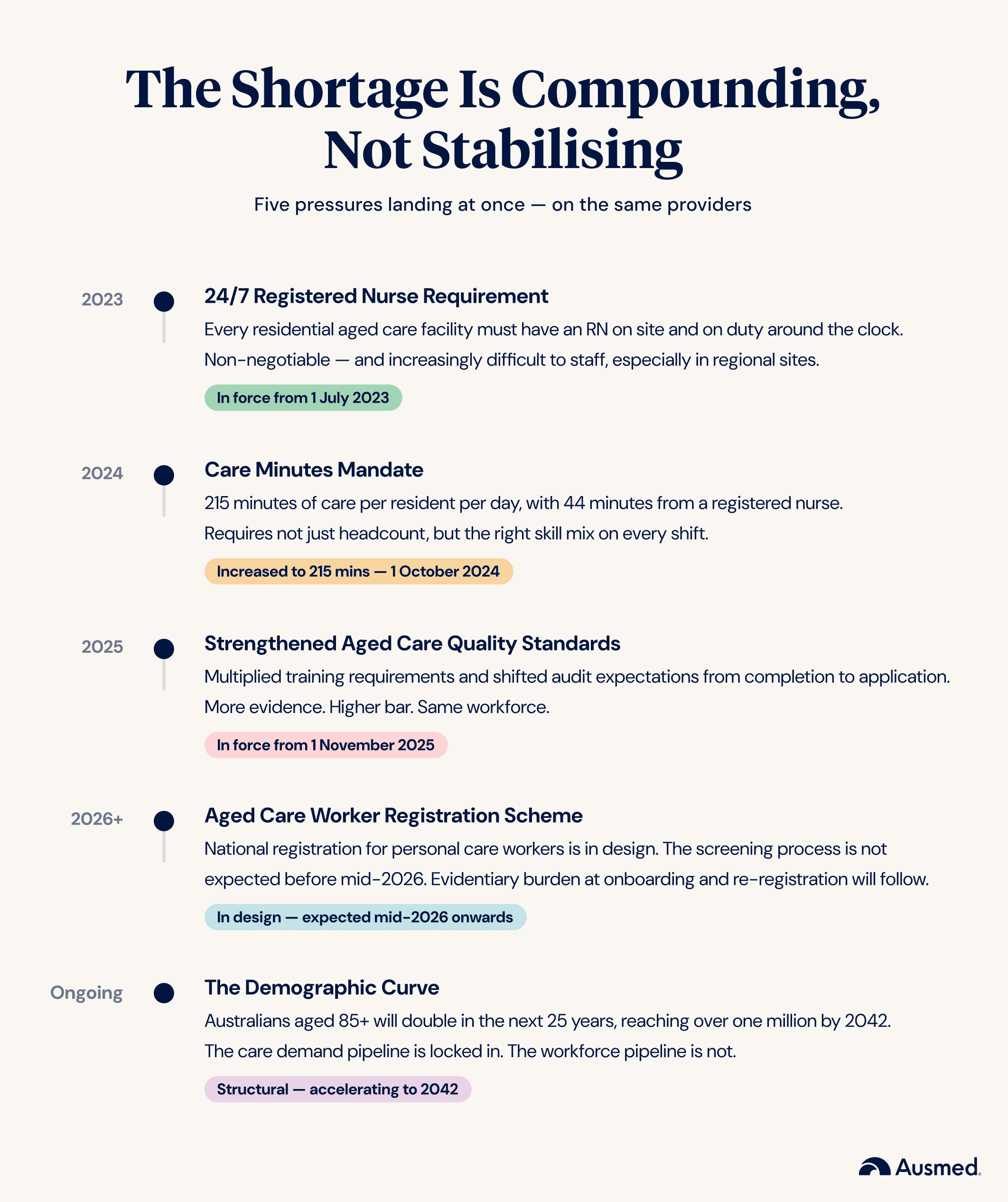
There are five concurrent pressures driving the gap.
The 24/7 RN requirement has been mandated since 1 July 2023. Every residential aged care facility must have a registered nurse on site and on duty 24 hours a day, 7 days a week, unless granted an exemption (Department of Health, Disability and Ageing, 2024a). It is non-negotiable but increasingly difficult to staff, particularly in regional sites. The exemption regime helps in narrow cases. It does not help at scale.
The care minutes mandate rose to 215 minutes per resident per day on 1 October 2024, of which 44 minutes must be delivered by a registered nurse (Department of Health, Disability and Ageing, 2025b). Providers can meet up to 10 per cent of the RN target (4.4 minutes) with care time delivered by an enrolled nurse (Australian Ageing Agenda, 2024). Meeting the mandate requires not just numbers but the right skill mix on every shift.
The Aged Care Worker Registration Scheme is in the consultation and design phase. National public consultation on a registration scheme for personal care workers ran from 18 February to 17 April 2025, with strong sector support for a phased rollout (Department of Health, Disability and Ageing, 2025c). The future aged care worker screening process aligned with the NDIS Worker Screening Check model is not expected to commence before mid-2026 (Department of Health, Disability and Ageing, 2025d). Providers should expect an evidentiary burden at onboarding and re-registration once the scheme is operational.
The Strengthened Aged Care Quality Standards, in force since 1 November 2025 alongside the commencement of the Aged Care Act 2024, have multiplied training requirements for many providers, and crucially, have shifted audit expectations from completion to application (Aged Care Quality and Safety Commission, 2025; Department of Health, Disability and Ageing, 2025a).
The demographic curve is unforgiving. As noted above, Australians aged 85 and over will double over the next 25 years, with that cohort reaching around one million by 2042 (ABS, 2023).
These pressures are not sequential. They are concurrent. A provider responding to the 24/7 RN requirement is the same provider preparing for the Worker Registration Scheme, and the same provider being audited against the new Standards. There is no breathing room.
The retention math no one is doing
The single most consequential conversation happening in aged care boardrooms in 2026 is the one about turnover cost. Most providers can quote their turnover rate. Few can quote what it costs them.
Industry analysts, including Josh Bersin and Gallup, consistently estimate the replacement cost of an experienced worker at 1.5 to 2 times their annual salary once recruitment, agency cover during the vacancy, onboarding hours, productivity ramp, and lost institutional knowledge are accounted for (Bersin, 2018; Gallup, 2019). The Society for Human Resource Management places the range more broadly at 50 to 200 per cent of annual salary, depending on role complexity (SHRM, 2022).
Aged care worker remuneration sits at the lower end of healthcare. Under the Aged Care Award (October 2025), direct care workers earn between \$1,182.80 and \$1,472.00 per week (roughly \$61,500 to \$76,500 annualised), and registered nurses earn between \$1,446.50 and \$2,542.40 per week (roughly \$75,200 to \$132,200 annualised) (Department of Health, Disability and Ageing, 2025e). Apply the 1.5x to 2x multiplier and the replacement cost of an experienced personal care worker is roughly \$92,000 to \$153,000, and of a registered nurse roughly \$113,000 to \$264,000.
That figure is the business case for retention investment. It is also the figure that most CFOs have never seen.
Three levers L&D actually controls
Not every retention lever sits with L&D. Pay scales sit with the CPO. Rostering sits with operations. Workplace culture sits with leadership.
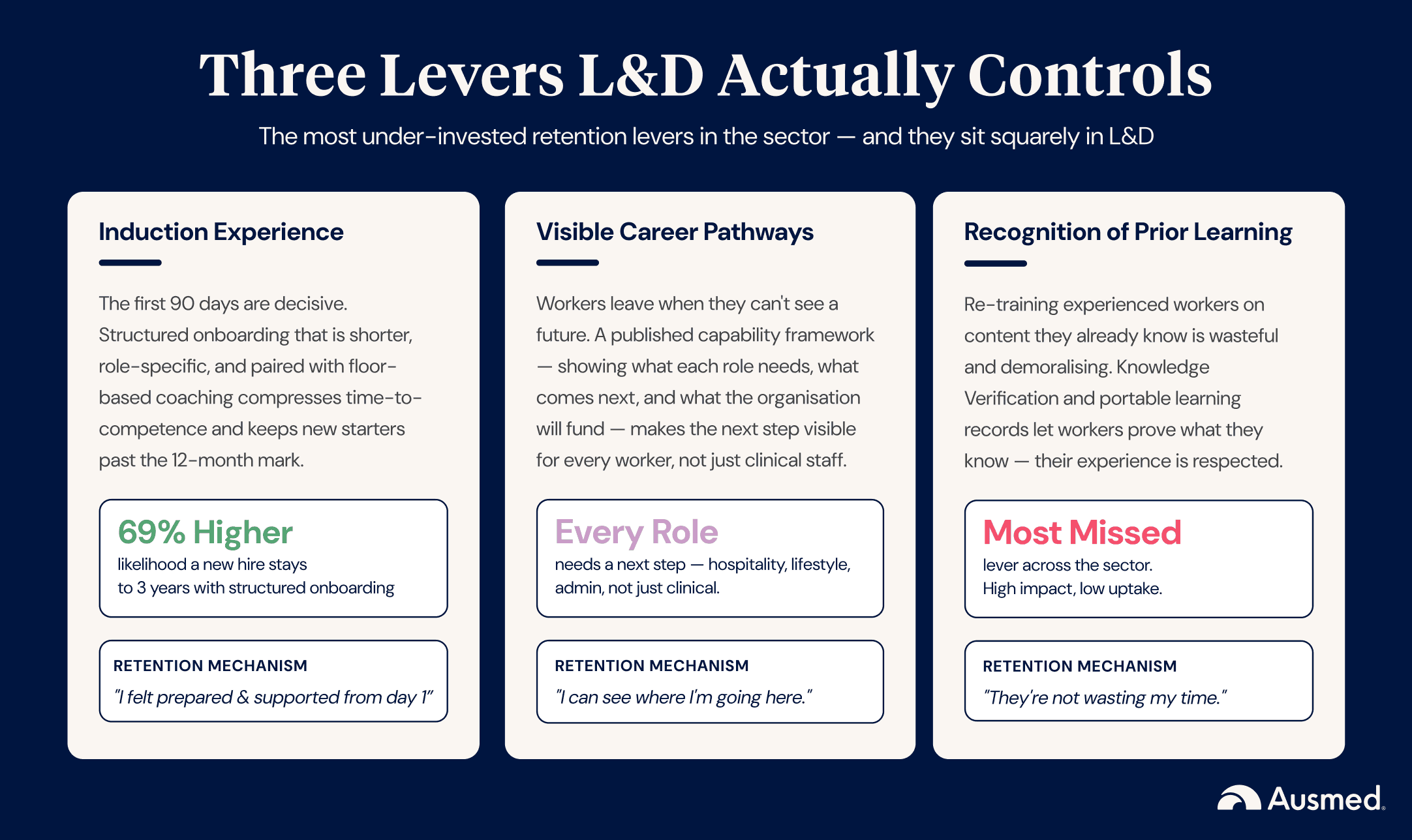
But three levers, three of the most consequential, sit squarely in the L&D function. They are also the three most under-invested in across the sector.
1. The induction experience
Research from Jobvite (2024) shows that approximately one in three new hires leaves within the first 90 days, and the Society for Human Resource Management reports that 20 per cent of all turnover occurs within the first 45 days (SHRM, 2022). Structured onboarding that extends through the first three months has been associated with a 69 per cent higher likelihood that new hires will still be in role at three years (BambooHR, 2024). In aged care specifically, the first 90 days of employment are decisive for whether a new starter will still be there at twelve months.
What "right" looks like in 2026: induction is shorter (12 to 16 hours of formal learning, not 40), more relevant to the worker's actual role and site, paired with structured workplace coaching, and explicitly designed to compress time-to-floor and time-to-competence.
What "wrong" looks like: a generic LMS bundle of compliance modules delivered in a sterile classroom, with no link to the work the new starter will actually do, and no clinical educator on the floor to follow up.
2. Visible career pathways
Aged care workers, particularly personal care workers, frequently describe their roles as dead-ends. They cannot see what comes next. The pathway from PCA to enrolled nurse to registered nurse exists, but it is rarely articulated, rarely supported with structured study time, and rarely modelled by the people they work alongside.
Providers who have built visible career pathways, with capability frameworks that show what each role requires, what the next role looks like, and what the organisation will fund to help workers get there, retain significantly more staff. The mechanism is simple. People stay where they can see a future.
3. Recognition of prior learning
The third lever is the one most often missed. When a worker moves between aged care providers, they bring a body of knowledge and experience that the new employer typically ignores. They are re-inducted, re-trained on the same modules, and required to demonstrate the same competencies they already demonstrated months ago at their previous employer.
This is wasteful, demoralising, and unnecessary. Knowledge Verification, a structured pre-assessment that allows experienced workers to demonstrate what they already know, addresses this directly. Industry-portable learning records like Ausmed Passport go a step further, giving workers a verified record of their training that follows them across employers.
The signal these tools send to experienced workers is simple: we know you already know this, and we're not going to waste your time pretending otherwise. That signal is a retention lever.
From workforce metric to board metric
The hardest part of the workforce conversation in 2026 is the framing. L&D leaders know intuitively that capability investment retains staff. They struggle to position that intuition as a board-level metric.
The opportunity is to reframe workforce capability data as a leading retention indicator, alongside the lagging indicators the board already sees (turnover rate, time-to-fill, agency spend).
Specifically, four metrics belong on the board agenda:
- Percentage of staff with a documented career pathway active in their development plan
- Average tenure by role, segmented by whether the worker has progressed through a capability level in the last 12 months
- Recognition-of-prior-learning credits redeemed per quarter (a proxy for experienced-worker engagement)
- Capability-framework coverage by role and site
These metrics belong in board papers next to financial performance and resident-experience data. They are the leading edge of the retention story. Providers who report them treat L&D as a strategic investment. Providers who do not, treat L&D as a cost line.
What good looks like in 2026
Across the providers we work with, five practices distinguish those who are pulling ahead from those who are falling behind:
- Shorter, role-specific induction. Not less induction, better induction. Less seat-time, more contextual relevance, more floor-time with clinical educators.
- A published, visible career pathway for every role. Not just clinical roles. Hospitality, lifestyle, administration. Every role has a next step, and every worker can see it.
- Knowledge Verification as standard practice. Experienced workers prove what they know. New workers complete the full module. Both are valid; the system distinguishes between them.
- A workforce capability framework that is actually used. Not a document on the shared drive. A living framework that drives training assignments, performance conversations, and rostering decisions.
- Workforce capability data on the board agenda. Quarterly. Trended over time. Linked to retention, audit performance, and resident-experience outcomes.
None of these are radical. All of them require a deliberate, system-level commitment. None of them survive on goodwill alone.
Where to start this week
For Chief People Officers and Heads of People: Ask your finance team to produce a turnover-cost number, applying the 1.5x to 2x salary multiplier. Take it to your next board meeting. Then audit your top three sites by tenure and identify whether induction quality, career-pathway visibility, or recognition of prior learning is the weakest lever.
For Heads of Quality and Risk: Map your audit-evidence requirements against your workforce capability framework. Where the two don't speak to each other, you are carrying duplicated effort and weakened evidence.
For HR Managers: Pull your 12-month tenure data, segmented by role and site. Where tenure is below sector average, run a structured exit-interview review for the past quarter.
For L&D leaders: Cost the time your team spends each month re-training experienced staff on content they already know. Take that number to your CPO as the business case for Knowledge Verification.
The workforce shortage in aged care is not a problem L&D can solve alone. But the levers L&D controls, induction, pathways, recognition, are the most under-invested across the sector. The providers pulling ahead in 2026 are the ones treating them as the strategic levers they are.
References
- Aged Care Quality and Safety Commission (2025) Strengthened Aged Care Quality Standards. Available at: https://www.agedcarequality.gov.au/providers/quality-standards/strengthened-aged-care-quality-standards (Accessed: 26 May 2026).
- Ageing Australia (2024) Workforce Strategy. Available at: https://ageingaustralia.asn.au/advocacy/workforce-strategy/ (Accessed: 26 May 2026).
- Australian Ageing Agenda (2024) 'Changes to care minutes target'. Available at: https://www.australianageingagenda.com.au/executive/changes-to-care-minute-target/ (Accessed: 26 May 2026).
- Australian Bureau of Statistics (ABS) (2023) Population aged over 85 to double in the next 25 years. Available at: https://www.abs.gov.au/articles/population-aged-over-85-double-next-25-years (Accessed: 26 May 2026).
- BambooHR (2024) The Definitive Guide to Onboarding. Available at: https://www.bamboohr.com/resources/guides/definitive-guide-to-onboarding (Accessed: 26 May 2026).
- Bersin, J. (2018) Employee retention now a big issue: Why the tide has turned. Available at: https://joshbersin.com/2018/04/cost-of-employee-turnover/ (Accessed: 26 May 2026).
- Committee for Economic Development of Australia (CEDA) (2021) Australia's dire shortage of aged-care workers requires immediate action. Available at: CEDA (Accessed: 26 May 2026).
- Department of Health and Aged Care (2024a) 2023 Aged Care Provider Workforce Survey. Available at: https://www.gen-agedcaredata.gov.au/resources/publications/2024/august/2023-aged-care-provider-workforce-survey (Accessed: 26 May 2026).
- Department of Health and Aged Care (2024b) Aged Care Worker Survey 2024 Report. Available at: https://www.health.gov.au/resources/publications/aged-care-worker-survey-2024-report (Accessed: 26 May 2026).
- Department of Health, Disability and Ageing (2024a) 24/7 registered nurse requirement. Available at: https://www.health.gov.au/our-work/care-minutes-registered-nurses-aged-care/24-7-rns (Accessed: 26 May 2026).
- Department of Health, Disability and Ageing (2025a) About the new rights-based Aged Care Act. Available at: https://www.health.gov.au/our-work/aged-care-act/about (Accessed: 26 May 2026).
- Department of Health, Disability and Ageing (2025b) Care minutes in residential aged care. Available at: https://www.health.gov.au/our-work/care-minutes-registered-nurses-aged-care/care-minutes (Accessed: 26 May 2026).
- Department of Health, Disability and Ageing (2025c) Consultation summary report on a national registration scheme to support personal care workers in aged care. Available at: DoHDA consultation summary (Accessed: 26 May 2026).
- Department of Health, Disability and Ageing (2025d) New ways of working in aged care. Available at: https://www.health.gov.au/topics/aged-care-workforce/new-ways-of-working-in-aged-care (Accessed: 26 May 2026).
- Department of Health, Disability and Ageing (2025e) Aged Care Worker Wages: Guidance for aged care providers. Available at: DoHDA wages guidance (Accessed: 26 May 2026).
- Gallup (2019) This Fixable Problem Costs U.S. Businesses $1 Trillion. Available at: https://www.gallup.com/workplace/247391/fixable-problem-costs-businesses-trillion.aspx (Accessed: 26 May 2026).
- Jobvite (2024) Recruiter Nation Report. Available at: https://www.jobvite.com (Accessed: 26 May 2026).
- Royal Commission into Aged Care Quality and Safety (2021) Final Report: Care, Dignity and Respect. Available at: https://www.royalcommission.gov.au/aged-care/final-report (Accessed: 26 May 2026).
- Society for Human Resource Management (SHRM) (2022) Understanding the Real Cost of Employee Turnover. Available at: https://www.shrm.org/topics-tools/news/talent-acquisition/real-costs-recruitment (Accessed: 26 May 2026).

